War on Diabetes newsletter 7th June 2026
Welcome to the nineteenth War on Diabetes newsletter - regular tips and ideas from someone who has had type 2 diabetes for six years and learned how to put it into remission. It's a practical and actionable guide to the kind of details that your doctor probably won't have time to tell you about.

May has been an exciting month - getting more steps and natural Vitamin D with all of the extra sunshine, but more importantly, attending the Public Health Collaboration (PHC) annual conference which marked their 10th anniversary. It was a pleasure to meet Dr David Unwin. I wanted to thank him for having the courage to prescribe CGMs for his type 2 diabetic patients. He has the rare success amongst UK GPs of having helped 157 of his patients reverse their type 2 diabetes. He's possibly the kindest person I've ever met and I found his humility and gift for listening to patients to help them find lifestyle solutions that worked really refreshing.
Find out how Dr. Unwin helped his patients reverse type 2 diabetes with his recent Diary of a CEO podcast interview with Steven Bartlett
Progress update
I've been making steady progress with stabilising my weight and getting my glucose levels back to where I want them - not perfect but going in the right direction. I'm nearly three months into using the Syai Ultra CGM and I'm finding it a lot easier to spot patterns over a longer period of time without obsessively checking readings throughout the day. I find the follow-up detail for each meal and the fortnightly reports make it easy to spot problems and also find successful strategies.
John o' Groats to Lands' End walking challenge
This summer, I'm walking the equivalent total distance of the length of the UK over five months. This is roughly 870 miles and works out at around 1.8 million steps.

So far I've managed over 400,000 steps since the start of May so I'm making good progress. On my nifty vibe-coded map following my virtual journey, I've just passed Bath in Somerset. I should be reaching Gloucestershire soon and will hopefully be starting on the Midlands early next week.
I'm fundraising for PHC because I feel that their low carb approach is a real game-changer for people who want to put type 2 diabetes into remission and their work will lead to changes needed to give future generations the option of remission instead of just management.
100 years of bad dietary advice for type 2 diabetes
My latest audiobook is 'Rethinking Diabetes' by Gary Taubes where he goes into the hundred-or-so year history of how we've ended up in a strange situation where relatively high carbohydrate diets are recommended for people with type 2 diabetes. He casually mentions as an aside, to a review by Theodore VanItallie on ketogenic diets, that scientists had observed that the human brain uses 100-150g of glucose (on a standard high carbohydrate diet) and that is the basis of the assumption that we need (at the very least) this amount to be provided by diet. This assumption is deeply flawed because it overlooks two crucial metabolic processes:
- The brain, along with most other organs and muscles, can switch to using more ketones in combination with less glucose once a person is reasonably fat-adapted (i.e. used to a low carbohydrate diet).
- Unless an individual is dangerously underweight, they can produce as much glucose as they need from stored body fat via a gluconogenesis - the liver (and to some extent the kidneys) can create new glucose through gluconeogenesis, primarily from glycerol released from body fat as well as some amino acids. That is how weight loss happens.
Despite the flaw in this old assumption, standard nutritional guidelines have been built upon it for decades. It is just widely stated that a balanced diet needs to contain approximately 200-350g of carbohydrates per day but no metabolic process is ever provided as to say why. Historically, this is also partly due to a fear of ketones - Diabetic Ketoacidosis (DKA) is what causes the acute risk of coma and death with any form of diabetes but it is important to understand that ketones in nutritional ketosis are nowhere near as highly elevated as they are in DKA. For reference, nutritional ketosis is where glucose levels are normal and ketones are typically around 0.5–3 mmol/L. I've had readings as high as 6.0 mmol/L and been fine. You only need to worry about DKA if ketones start climbing above around 10 mmol/L and glucose levels are high - that is a medical emergency.
Prior to the first use of insulin therapy in 1922, which saved 14-year old Leonard Thompson from dying due to type 1 diabetes, type 2 diabetes had previously been typically treated with a high fat, low carbohydrate diet. Insulin was a miracle breakthrough in driving down the high blood glucose levels for type 1 and it was also found to be effective at reducing levels for people with type 2. This is where the folly of chasing a single biomarker comes in. Type 2 diabetes is primarily a condition of chronically elevated insulin, not too little insulin. Chasing the downstream effect of increased blood glucose for type 2 puts more strain on the mitochondria and increases insulin resistance - making the underlying condition worse and a cycle of ever increasing insulin doses being required.
The effects of suppressing ketosis
Dr. Isabella Cooper gave a presentation at the 2026 PHC conference that had some quite striking statistics. The burden of proof for the safety of ketogenic (high fat, low carb) diets has been unfairly set higher than the low fat, high carbohydrate diet advice that we have all been fed since the 1960s. There is no large scale randomised control trial that proves that low fat, high carbohydrate diets are safe but their advocates insist that one is provided for the alternative before ketogenic diet can be recommended. Performing these types of studies on a large scale is notoriously difficult and expensive because there are so many confounding factors that are almost impossible to eliminate over a group of people for decades - how do you know they're not smoking, drinking alcohol or eating donuts etc.? The idea that saturated fat clogs arteries has never been proven to be true - it's an outdated assumption and Dr. Cooper's study adds to the growing body of evidence that it's quite drastically wrong...
The 'Effects of Suppressing Ketosis' study was an experiment that flipped the usual testing order around. Instead of going from low fat, high carb to a ketogenic diet, Dr. Cooper chose to select participants that were already consuming a ketogenic diet and then put them on the standard low fat, high carbohydrate diet for 21 days. The participants had several biomarkers checked at three intervals: 21 days of being on their usual ketogenic diet, 21 days of being on the low fat, high (270g) carbohydrate diet, and finally, another 21 days of being back on their normal ketogenic diet.
Here is a summary of just a few of the average biomarker changes. I'll breakdown the details of what each marker means but all of these increases are essentially signs of metabolic distress.
- HOMA-IR more than doubled from 0.97 to 2.07
- IGF-1 increased from 149 to 273 ng/ml
- Leptin more than tripled from 4.50 to 15.08 ng/ml
- ALT:AST ratio increased from 0.74 to 0.96
HOMA-IR more than doubled from 0.97 to 2.07
HOMAR-IR is a measurement of insulin resistance calculated by multiplying fasting insulin by fasting glucose level. The higher the number, the more insulin resistance is present - the fundamental metabolic problem of type 2 diabetes - insulin is chronically too high but is being rejected by the body's cells due to oxidative damage.
"Too much insulin, basically ages you. That's what it does. It damages your mitochondria and ages you." Dr. Isabella Cooper
Less than 1.0 means you are insulin-sensitive which is optimal.
Above 1.9 indicates early insulin resistance.
Above 2.9 indicates significant insulin resistance.
https://thebloodcode.com/homa-ir-calculator
So an increase in otherwise healthy people over a space of 21 days from 0.97 to 2.07 means that they're already on their way to developing prediabetes.
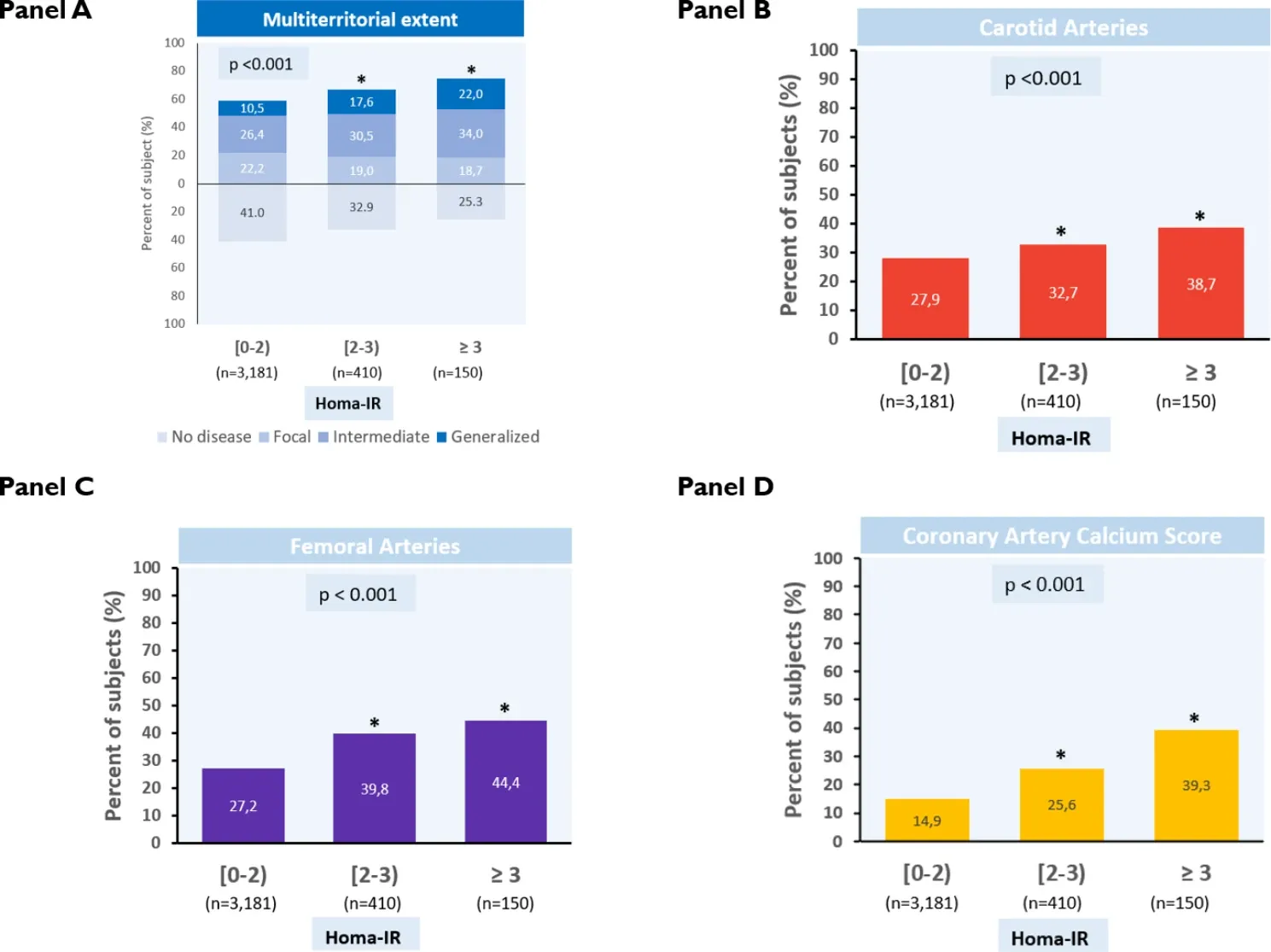
Dr. Cooper also references the cardiovascular disease risk implications from a study which looked at subclinical cardiovascular risk factors associated with varying HOMAR-IR. Look at Panel D below which shows coronary artery calcium (CAC) - a measure of how much subclinical atherosclerosis is occurring in arteries. This increases from 14.9 for a HOMA-IR below 2, to 25.6 for those above 2. So this suggests a significantly increased risk of cardiovascular disease.
IGF-1 increased from 149 to 273 ng/ml
Insulin-like growth factor 1 (IGF-1) is a powerful hormone that is similar to insulin, in that it promotes growth and energy activation. It is around 1000 times more potent than insulin so it has significant effects even in small amounts. It is also regulated by insulin so having chronically elevated insulin as is the case with type 2 diabetes can lead to an increased risk of cancer as well as making insulin resistance worse. Dr. Cooper suggests an optimal range for IGF-1 as 120-160 ng/ml. Being above or below that range is a risk factor for disease. The average 273 ng/ml range for the participants in the study is associated with the following increase in relative cancer risk (if this level was maintained over a longer period of time):
- 69% colon cancer
- 49% prostate cancer
- 65% breast cancer
- 106% lung cancer
Leptin more than tripled from 4.50 to 15.08 ng/ml
Leptin is a key satiety hormone released by fat cells but it starts to become ineffective with chronically high levels. Once it starts to reach levels above approximately 15 ng/ml it is associated with increased adiposity (weight gain) because the brain becomes leptin resistant - it stops acknowledging leptin's "we've still got plenty of energy stored as fat" signal. This is part of what Professor Richard Johnson calls the 'survival switch' that initiates foraging behaviour - we've evolved to eat as much sugary fruit as possible at the end of Summer and during Autumn in order to fatten up in preparation for the scarcity of winter. It also has an evolutionary benefit during puberty and pregnancy due to the increased need for tissue growth. Insulin is also the primary driver of leptin release so it makes sense that higher carbohydrate consumption leads to increased leptin. It suppresses apoptosis - the breakdown of cells needed for the replacement of damaged cells (that's not good for clearing potentially cancerous cells), and when chronically elevated it is associated with higher coronary artery calcium (CAC) - the atherosclerosis leading to heart attacks. Higher leptin levels are also associated with an increased risk of incident frailty i.e. older people being injured by a fall.
ALT:AST ratio increased from 0.74 to 0.96
Alanine aminotransferase (ALT) is an enzyme that signals liver damage. Aspartate aminotransferase (AST) is another enzyme produced by many organs that speeds up some chemical reactions in the body. Dr. Cooper suggests an ALT:AST ratio of below 0.8 is considered optimal whereas being over 0.8 is associated with hyperinsulinemia - HOMA-IR being over 2.0 and prediabetes being on its way. Increased carbohydrate consumption is associated with a higher ALT level which is why the ratio increased above the 0.8 threshold.
Key take-away
These participants were on a very healthy version of the standard low fat, high carb diet. They were told to go for "starches, not sugar". Their readings did come back down to almost their initial ranges in the final 21 day period of going back to their ketogenic diet, so their overall risk for developing disease from the low fat, high carb diet is going to be negligible. However, this would not be the case for someone eating this way for decades of following the standard dietary advice. Sadly, we've now normalised the consumption of excessive amounts of ultra processed food, refined grains and sugar to the point where we're facing a pandemic of metabolic disease around the world.
Personally, I've taken Dr. Cooper's presentation as an inspiration to go more keto. In practical terms this means I'm going to be trying out a new method of 'dirty fasting' for two days a week. I find a full clean water fasting day quite difficult because I find it hard to concentrate and I become even more irritable than usual. I'm going to try butter coffee for breakfast and a bone broth drink for lunch - both very low protein and almost zero carbohydrates. An interesting early observation is that on one of my morning gym sessions my blood glucose barely nudged up at all. I would normally go up to around 10 mmol/L by the end of a gym session but the day after my butter coffee/bone broth day, even with a full evening meal, my glucose didn't rise higher than 6.6 mmol/L. That's showing I've probably become more fat-adapted and/or have managed to keep my glycogen stores lower than usual. My new goal is to get into the habit of doing this two days a week.

Food devils
Premier Inn sausages
Three egg, three sausage, three bacon is my usual buffet breakfast option (tomatoes and mushrooms are also welcome). It might seem excessive but it means I can skip lunch when out and about. Sausages are one of the few things I generally recommend to get from a supermarket instead of a butcher's as they can contain sugar, flour and other carbohydrate fillers. In a supermarket you can check the ingredients list for UPF nasties and also review the sugar content - anything above 1% sugar goes back on the shelf. I risked the Premier Inn breakfast sausages while staying in London for the PHC conference and my glucose levels shot up by 3.9 to 9.6 mmol/L which is a lot for a breakfast.

Belgian beer
I have a two-pint-per-week limit on beer and certainly don't recommend it for anyone with type 2 diabetes. I'd had this as a treat for surviving the train chaos of getting to London and back. This took me up to 11.8 mmol/L and stayed there most of the night. Not recommended!

Food heroes
These might seem weird but don't knock it 'till you try it. These have been a game-changer for my fasting regime and kept my glucose levels at around 5.5 mmol/L all day. I'm going to be doing more of these days and monitoring ketones to see if this is an effective fasting cheat for getting into nutritional ketosis.
Butter coffee (breakfast)
Okay it's still some calories but I find this can stave off hunger all morning so it's a good breakfast option on my dirty fasting days - munchies at bay until at least 11.30 am. I also tried it with coconut oil instead - don't do that - it tastes really weird. If this is a bit too extreme to start with, try adding cream or milk to take the richness edge off.

Bone broth (lunch)
I use Jarmino organic bone broth. I'm all for making your own broth by boiling bones for hours but it's quite a messy and time-consuming effort, so adding half a teaspoon of this concentrated broth to hot water is a quick and easy lunch option. I'm still working on perfecting the recipe for this. I liked a version with soy sauce but am currently avoiding that due to thyroid issues so I've found cider vinegar is a good alternative to add some tang. It's best to add soft-leafed herbs such as parsley, coriander, or fenugreek rather than rosemary which can be a bit gritty.

Sponsored*
Bitter melon & cinnamon tea
While fasting, herbal (or at least no dairy) teas help to relieve hunger niggles without breaking a water fast. A friend on the PHC course recommended bitter melon for help with glucose control so I decided to try this Nutra Glycemia tea and it's my new favourite for when I can't be bothered with the preparation steps for my BDNF-boosting tea with its multiple ingredients. The cinnamon and fenugreek form a well balanced sweet and earthiness. This one is now part of my daily routine whether I'm having a fasting day or not.
Shirataki noodles

Shirataki noodles (not to be confused with shitake mushrooms) are super-low-carb noodles. They are made from konjac root (no, not the brandy - it's Southeast Asian elephant yam root). I add them to my regular pork ramen and they work well with a chicken curry as well.


